Ozempic Face: What GLP-1 Drugs Actually Do to Your Skin
Ozempic face is now in peer-reviewed medical literature. GLP-1 receptor agonists deplete facial fat and alter adipose-derived stem cells, producing hollowing and laxity that reads differently on brown skin. Here is the mechanism, why the standard correction advice carries PIH risk, and what the rese
TL;DR
- "Ozempic face" is now in peer-reviewed literature. GLP-1 receptor agonists cause rapid loss of facial subcutaneous fat and dermal white adipose tissue, producing hollowing, laxity, and accelerated-looking aging that is distinct from ordinary diet-related weight loss.
- The mechanism goes beyond caloric deficit. GLP-1 agonists alter adipose-derived stem cells (ADSCs), which are structurally critical for skin renewal and collagen support. Losing facial fat this way is not the same as losing it through diet alone.
- A 2026 randomized controlled trial in 25 GLP-1 RA users found a topical firming regimen produced 44% reduction in skin laxity versus placebo over 12 weeks.
- On brown skin, volume loss appears as deepened shadows rather than surface wrinkles, and energy-based correction procedures carry real hyperpigmentation risk. The topical-first strategy is both evidence-based and categorically safer.
- Oral collagen peptide supplementation at 5g per day has 12-week RCT-level evidence for improving dermal density and skin firmness.
"Ozempic face" entered peer-reviewed medical literature in 2025, which means it is no longer just an internet complaint. It has a documented mechanism, a clinical name used by surgeons and dermatologists, and a growing body of research on how to manage it. If you are taking semaglutide, tirzepatide, or any GLP-1 receptor agonist for weight management, and you have noticed your face looking hollowed, more shadowed, or older than you expected at your current weight, you are not imagining it. What is happening at the tissue level is distinct from normal dieting-related fat loss, and it matters especially for melanin-rich skin, where volume loss reads differently and correction procedures carry risks that standard recommendations will not account for.
What Ozempic Face Actually Is
"Ozempic face" describes a cluster of facial changes that occur specifically in people using GLP-1 receptor agonists: facial volume loss, skin laxity, deepened nasolabial folds and marionette lines, and a hollowing that ages the face beyond what the weight loss itself would predict. A 2025 review published in HNO by Seidel and Bode catalogued these changes directly, describing volume loss, skin laxity, and pronounced wrinkles as the defining triad in patients using GLP-1 medications for off-label weight reduction, and used the term "Ozempic face" as an established clinical descriptor (Seidel 2025).
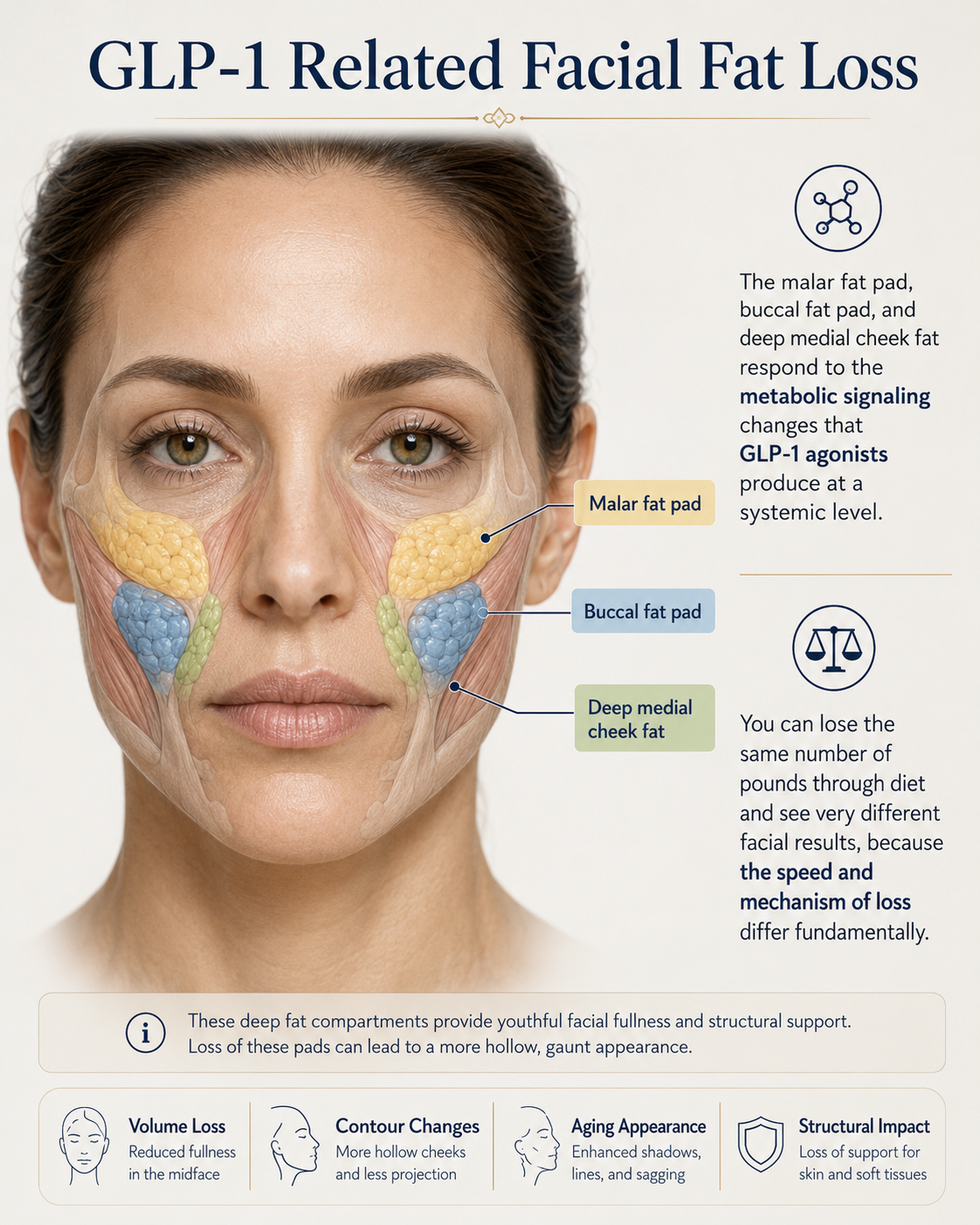
The phenomenon is now distinct enough that it is routinely differentiated from the facial changes of ordinary caloric restriction. The rate of fat loss on GLP-1 medications is faster, and the facial fat compartments are particularly vulnerable because they are hormonally sensitive. The malar fat pad, buccal fat pad, and deep medial cheek fat respond to the metabolic signaling changes that GLP-1 agonists produce at a systemic level. You can lose the same number of pounds through diet and see very different facial results, because the speed and mechanism of loss differ fundamentally.
The Mechanism Goes Deeper Than Fat Loss
The standard explanation for ozempic face is that rapid weight loss depletes facial fat. That is true but incomplete. A 2024 review in Aesthetic Surgery Journal by Ridha et al. offered a more precise mechanistic account: the accelerated facial aging observed in GLP-1 RA patients appears to be multifactorial, involving loss of dermal and subcutaneous white adipose tissue, altered proliferation and differentiation of adipose-derived stem cells (ADSCs), and impacts on the production and secretion of hormonal and metabolic factors (Ridha 2024). These changes compromise the structural integrity and barrier function of the skin, and may additionally contribute to diminished facial muscle mass.
The ADSC component is the part that consumers mostly misses. Adipose-derived stem cells are not passive inhabitants of facial fat. They are active contributors to skin renewal, collagen production, and the structural maintenance of the dermis. When subcutaneous fat is rapidly depleted, the ADSC population depletes alongside it. This is categorically different from gradual aging-related fat redistribution, where some ADSC-driven repair capacity is maintained over time. Rapid GLP-1-mediated fat loss removes the stromal support system for the overlying skin faster than the skin can adapt structurally.
A 2026 review in the Journal of Craniofacial Surgery by Bariskan et al. confirmed that the cosmetic consequences of GLP-1-induced rapid weight loss include skin laxity, facial volume loss, and compromised skin elasticity as a combined outcome (Bariskan 2026). The skin does not simply contract to fit a smaller facial volume underneath it. It hangs, because the fat that gave it structural support is gone, and the cellular machinery that would normally signal repair and remodeling has been depleted with it.
Why Volume Loss Reads Differently on Brown Skin
Skin laxity and facial hollowing present visually differently on melanin-rich skin, and almost none of the clinical literature on GLP-1 aesthetics addresses this directly. Most ozempic face photos circulating in both consumer media and clinical case presentations feature lighter skin tones, which shapes the conventional clinical picture in ways that do not translate accurately to Fitzpatrick IV through VI.
On lighter skin, volume loss typically manifests as visible surface wrinkling and fine lines that respond well to resurfacing and skin-tightening procedures. On brown and deeper skin, where the dermis is denser, and the surface does not crinkle the same way, volume loss manifests primarily as deepened shadows. The tear trough looks darker. The nasolabial region creates a shadow that reads as a dark crescent rather than a fold. The under-eye area may appear hyperpigmented when the structural tissue that was supporting it from underneath has been depleted. These shadows are not pigmentation in the traditional sense. They are structural, caused by the geometry of deflated tissue beneath melanin-dense skin.
The practical implication is that standard product and procedure recommendations for ozempic face correction may address the wrong problem on brown skin. Volume replacement rather than surface treatment is the primary intervention needed.
What the Research Shows Actually Helps
The most clinically actionable recent evidence for topical intervention in GLP-1 RA users comes from a 2026 randomized controlled trial by Moradi et al., published in Dermatology and Therapy. The study enrolled 25 GLP-1 RA users with Fitzpatrick II through VI skin in a split-face design, comparing a topical regimen featuring Proxylane and wild fruit flavonoids against placebo over 12 weeks, with a single focused ultrasound session at week 4. At 4 weeks of topical-only use, the regimen produced statistically significant reductions in facial skin laxity and marionette lines versus placebo. By week 12, the combined protocol achieved 44% reduction in skin laxity and 34% reduction in marionette lines, with 94% of subjects reporting moderate-to-significant improvement (Moradi 2026). The inclusion of Fitzpatrick V and VI participants makes this one of the few GLP-1 skin studies with direct relevance to melanin-rich readers.
For internal support, oral collagen peptide supplementation has credible evidence behind it. A 2025 double-blind placebo-controlled trial by Wang et al. in the Journal of Cosmetic Dermatology enrolled 77 participants supplementing 5g per day of bioactive collagen peptides for 12 weeks. Compared to placebo, the collagen group showed significant improvements in dermal density, skin hydration, and transepidermal water loss, and these effects were maintained through a 4-week washout period, suggesting structural rather than surface-level changes (Wang 2025). Collagen supplementation is systemic, generates no heat, and carries no hyperpigmentation risk regardless of skin tone. For someone managing ozempic face on brown skin, it is the most accessible starting point with the broadest safety profile.
Protein intake and resistance training are the upstream variables most consistently cited in the clinical literature as protective against excessive facial muscle and volume loss during GLP-1-induced weight loss. The mechanism is simple: preserving lean mass during weight loss reduces the proportion of structural tissue lost alongside fat. Adequate protein targets of 1.2g per kilogram of body weight daily are the general clinical recommendation during weight loss on these medications.
The Products Worth Using While You Navigate This
The intervention approach for ozempic face works in two layers: internal support for collagen and dermal structure, and topical work to address laxity at the skin surface. Microcurrent devices address the muscle toning layer without generating heat, making them appropriate for brown skin without PIH risk. For the collagen and topical firming layer, the products below represent the most evidence-adjacent options currently available without a clinical visit.
| Product | Type | Best For | Price |
|---|---|---|---|
| Vital Proteins Collagen Peptides | Oral supplement, hydrolyzed bovine collagen | Dermal density support, systemic, no PIH risk | ~$27 |
| The Ordinary "Buffet" Multi-Technology Peptide Serum | Topical multi-peptide complex | Topical firming, layerable under SPF, accessible | ~$17 |
| NuFace Mini+ | Microcurrent device, 200 microamps, app-guided | Facial toning without heat, zero PIH risk on brown skin | ~$179 |
| L'Oreal Revitalift 1.5% Pure Hyaluronic Acid Serum | HA plumping serum | Surface hydration and volume-depleted skin, daily use | ~$33 |
On the Vital Proteins: the serving size is 20g collagen per scoop, higher than the 5g dose used in the Wang 2025 trial. Starting at 5 to 10g daily is a reasonable entry point. Unflavored collagen peptides dissolve into coffee or smoothies without changing texture. Any brand supplying hydrolyzed bovine or marine collagen peptides at 5g or more per serving achieves the same endpoint, so if you prefer a different format or brand, the dose and consistency matter more than the specific product.
On the NuFace Mini+: if you are new to microcurrent, the SkinDecoded microcurrent guide covers the clinical evidence and technique in detail. The short version is that consistent use five days per week for 60 days is the standard loading protocol, and results are cumulative. It fits into the same evening routine as your peptide serum, applied after skincare has fully absorbed.
Honest Caveat: Topicals Have a Ceiling Here
Topicals and supplements will not replace lost facial volume. If you are a year or more into GLP-1 use with significant depletion in the malar and buccal compartments, no collagen supplement or firming serum is going to restore what was structural fat. The evidence-supported correction for significant ozempic-related facial volume loss is volume replacement: hyaluronic acid fillers for immediate volumization, polynucleotide or PDRN biostimulators for longer-term ADSC stimulation, and autologous fat transfer for the most complete structural restoration. A 2024 review in the Journal of Cosmetic Dermatology by Haykal et al. reviewed each of these modalities in the context of GLP-1 patients specifically, identifying biostimulatory agents targeting ADSC function as the most mechanistically rational approach for this patient group, and calling for personalized multimodal strategies (Haykal 2024).
For brown-skin patients considering any correction procedure: find a practitioner who can show documented results on Fitzpatrick IV through VI skin, not just before-and-after photos from lighter-skinned populations. Radiofrequency and HIFU generate heat in the dermis, and heat-based devices carry real PIH risk on melanin-rich skin. Fillers placed correctly by an experienced injector do not trigger PIH. The injection trauma itself is manageable; the choice of energy-based device procedure is where the risk concentrates for darker skin. If you are uncertain, topicals, collagen support, and microcurrent for the first six months give you time to evaluate the trajectory before committing to a clinical procedure.
Newsletter
A calmer read before your next purchase.
One weekly note on skincare trends, product claims, and how to choose with more context.


